


The Ballad of Mr. Blue - part 1
Dizziness, differentials, and a dumbfounded student

This is a change of pace from my usual writing here on “Building Docs.” What follows is the first part of a series involving one of my first, and most memorable, patients - Mr. Blue. Over the course of the next couple weeks I’ll walk you through the case, Mr. Blue himself, and the lessons learned while caring for him on the medical wards. I hope you enjoy the story and learn something in the process!
If you have yet to subscribe, consider subscribing FOR FREE by hitting the button below! As always, if you wish to support me and my work, hit that like button, comment, or share this article with friends and family. Thanks!
_________
Dizziness
Who is Mr. Blue?
Mr. Blue was one of my first patients when I worked on the inpatient medical service during my internal medicine rotation. (No, his name is not actually Mister Blue). It was my first month of “practicing medicine” in a hospital. He was a 50–60-year-old man with a history of a prior stroke and heavy alcohol use.
What problem is Mr. Blue experiencing?
He was sitting in his apartment, got up to shave, and shortly after starting to shave he felt lightheaded and dizzy, and he fell. He called out to his neighbor for help because he couldn’t get up afterward. He’s unsure if he lost consciousness, but was/is worried because he cannot walk properly since falling. He could walk normally beforehand…and now he can’t walk at all. That’s why he got himself to the emergency department.
How do we solve Mr. Blue’s problem?
To solve this we need to talk about the “differential diagnosis”. Your differential diagnosis, abbreviated DDx for short, serves as a list of potential diagnoses that could explain your patient’s symptoms. It’s important to start your list as wide as possible to narrow it as you gather more clinical clues from your patient via history-taking, exam findings, and different diagnostic tests. In other words, you got to cast a wide net to catch the right fish.
But how do you do that? Especially with Mr. Blue, where his symptoms are vague and nonspecific to any disease. To hammer this point home for you, let’s play a game with some classic presentations of common diagnoses. Let’s see how you do (Answers are below)
12-year-old kid, acute onset shortness of breath, wheezing, intermittent cough, use of accessory muscles to breathe, has allergies and eczema —> diagnosis?
55-year-old man, acute dull constant chest pain that now radiates to his jaw and down his left arm, profusely sweating and nauseous, history of high blood pressure and diabetes —> diagnosis?
30-year-old woman, nausea, low back pain, breast tenderness, increased cramping, increased frequency of urination, and she hasn’t menstruated —> diagnosis?
60-year-old man, presents with resting tremor of his right hand, general slowness of movement, rigidity, unable to maintain a stable posture, slow and shuffling gait —> diagnosis?
35-year-old woman, increased sweating, heat intolerance, palpitations, anxiety, weight loss despite normal appetite, protruding eyeballs —> diagnosis?

Here’s a famous doctor to inspire you…
_________
Answers
1) Asthma, or acute asthma exacerbation
2) Heart attack, or “myocardial infarction” until proven otherwise
3) Pregnancy… congratulations!
4) Parkinson’s disease
5) Graves disease (Hyperthyroidism is acceptable, too)
How’d you do?
5/5 = House, MD
4/5 = Dr. Quinn, Medicine Woman
3/5 = Doogie Howser, MD
2/5 = Leslie Nielsen in the 1980 classic film “Airplane!”
0-1/5 = Eg-no-ra-moose :)

Great movie…ok let’s get back to Mr. Blue
_________
Differentials
Let’s boil this case down to its nuts and bolts. A 50-60-year-old man with a history of stroke and alcohol use has a syncopal episode and resultant ataxia (fainting and abnormal gait). There could be one reason causing these symptoms, or there could be more than 1 thing going on. Either way, no diagnosis is jumping out to us like the mini-cases we worked through above. So…let’s make our DDx.
There exist 1,000,001 ways of making a DDx, but one of the first ways we’re taught is with the acronym “VINDICATE.”

Let’s briefly go through some of the potential diagnoses that we need to think about with Mr. Blue. DISCLAIMER: in the interest of time this is not a complete differential, just an example of some of the things for which our team looked out.
Vascular - First thing that we need to rule out is a stroke, especially with his history of a previous stroke and current gait impairment. So, we’d need to get a CT scan and ECG right away (which the good people in the emergency department did). ECG can also rule in/out an arrhythmia that could cause lightheadedness and a fall. An arrhythmia itself wouldn’t explain his difficulty walking, though. A carotid artery duplex (ultrasound of your neck blood vessels) and echocardiogram (ultrasound of your heart) are also useful tools when working up a potential stroke. Another vascular thing to think about would be Carotid Sinus Hypersensitivity or Carotid Sinus Syndrome.
Carotid Sinus Hypersensitivity?
There are small pressure sensors in the main artery of your neck. If they experience external pressure – like while shaving or tightening a necktie – they can trigger a drop in your blood pressure, resulting in dizziness and a fall.
However, this still wouldn’t explain his difficulty walking. Maybe there’s more than one thing going on…let’s keep building out our DDx.
Infection – he could have a bug! However, you would expect to see other clues pointing towards this, eg runny nose, trouble breathing, cough, sick contacts, high temperature, etc.
Neoplastic – a brain tumor is lower in likelihood and something that isn’t needed to be ruled out immediately, but it is something that could cause a seizure, which would be on our DDx. However, a brain tumor would be visualized on head imaging. Things going against seizure are a lack of history of confusion and drowsiness after falling, otherwise known as a postictal phase. Additionally, biting your tongue and losing control of your bladder isn’t uncommon during a seizure, and Mr. Blue didn’t present with either of these signs. However, it’s important to note that the absence of clinical evidence for a disease doesn’t mean that the disease itself is absent.
Degenerative/Deficiency – there could be both degenerative disease or vitamin deficiency contributing to his gait abnormalities. Vitamin B12 deficiency over time can cause difficulty walking, called Subacute Combined Degeneration. Degenerative disease would entail degeneration of the cerebellum, the center of your brain that coordinates movement. These include Cerebellar Degeneration caused by excessive alcohol use, or his walking could also be a part of a disorder called Wernicke’s Encephalopathy (W.E.). W.E. is common in those with chronic alcoholism and is linked with a thiamine deficiency (vitamin B1). The classic triad of symptoms includes gait ataxia (abnormal walking), encephalopathy (disorientation, inattentiveness, etc), and oculomotor dysfunction (trouble with eye movements).
Idiopathic/intoxication/iatrogenic – Mr. Blue could’ve simply been dehydrated which caused him to feel faint and fall. But again, it wouldn’t explain his walking issues. Alcohol intoxication could explain the dizziness, fall, and trouble walking immediately afterward (if Mr. Blue was still intoxicated). However, it wouldn’t explain a consistent problem walking unless there was a degenerative component, like the previously mentioned Alcoholic Cerebellar Degeneration or Wernicke’s Encephalopathy.
And so on… you get the idea.
Another way to look specifically at his “syncopal episode” is by trying to discern if it is cardiac related, nervous system related (like the carotid sinus hypersensitivity), or related to orthostasis (which occurs when you’re unable to maintain your blood pressure when you stand or change positions). Here’s an excellent chart from the American Academy of Family Physicians on the causes of syncope.

The bottom line is that, as Dr. Meador points out in Rule 83 of his book - You cannot diagnose what is NOT in your differential diagnosis.
_________
Any more clues regarding Mr. Blue?
Vitals - generally normal; evidence of orthostatic changes (lower blood pressure when standing), but not consistent enough to meet criteria for “orthostatic hypotension.”
Physical exam - normal except for his neurological exam. Generally speaking, Mr. Blue had a resting tremor in his upper extremity, abnormal sensation, abnormal gait and impaired coordination of his lower extremity, intermittent resistance to passive movement, and abnormal reflexes in the lower extremities (the specifics of which I do not remember, sorry).
Labs - some abnormalities, but nothing too out of the ordinary or specific. Blood alcohol level was normal.
Imaging - CT scan of the head showed no abnormalities, no evidence of stroke. ECG showed no abnormalities on admission and was normal throughout his stay. Imaging otherwise was normal.
Other tests - Of the additional tests we ordered, one was positive. That was the “tilt-table” test, a test meant to reproduce a fainting episode by changing your body position. Though for someone of Mr. Blue’s age, it’s not uncommon to garner a false-positive with this test.
Hmmm…what do you think?
_________
Dumbfounded
A couple of days go by and we’re a little closer to explaining Mr. Blue’s symptoms, but not by much. It’s a confusing case and, the longer he stays in inpatient for observation, the more his symptoms start to become…inconsistent. Nonetheless, our team powers forward, racking our brains trying to figure out the cause of Mr. Blue’s puzzling state. There is some evidence for both a vasovagal and orthostatic cause of his syncope. As far as the difficulty walking…well, we’re not quite sure. It could be a few different things or a combination of those things. So far, our emphasis is on observing him, providing the appropriate supportive care, and consulting other departments for help (like neurology and PM&R). Medicine is a team sport.
One of the benefits as a student working on a great medical team is that they encourage and support you to dive deep into your patients and their symptoms. So, with the support from the residents and attendings with which I worked, I swung for the fences and tried my best to figure out the correct diagnosis.
What was your diagnosis, Tyler?
What in the world is that?
It’s a rare disease that can be understood as “Parkinson’s plus,” meaning that it is comprised of Parkinson’s-like symptoms that also involve the autonomic nervous system (the part of your nervous system that controls involuntary body processes, like blood pressure).
What was your evidence?
Mr. Blue had many symptoms reminiscent of Parkinson’s disease. For example, he had a tremor of his hand at rest. Additionally, his extremities were somewhat resistant to passive movement, i.e. rigidity. But what convinced me was watching him attempt to walk. Usually, those with Parkinson’s disease have a slow, shuffling gait. With Mr. Blue, it was certainly slow, but it was almost like he was afraid to put weight on his feet. He couldn’t pick his feet up and/or coordinate them. In my vast experience working in inpatient medicine (at that point in time, totaling 11 days) I had never seen anything like it. Place this in the context of a positive tilt-table test and evidence for orthostatic hypotension; that ticks the “autonomic” part of the diagnosis.
The next step, I thought, could be to get an MRI of his brain to look for any signs that supported this diagnosis (eg the “hot cross bun” sign). I presented my findings and thoughts to my team, and then to my attending. He kindly stated that though this disease is rare, there was enough here to investigate further, so he went ahead and ordered an MRI for Mr. Blue.
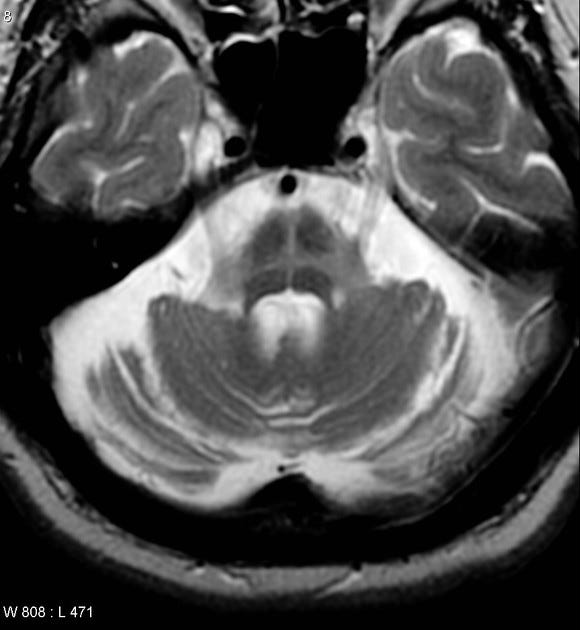
Here’s the “hot cross bun” sign in a patient with MSA, courtesy of radiopaedia.
I was elated! I felt great about the work that I did. I thought (or hoped, rather) that I hit a hole-in-one…but that feeling ended just a few of hours later. The MRI had been canceled by the neurologist familiar with Mr. Blue. He didn’t need it.
I realized I did NOT, in fact, hit a hole-in-one. Rather, I was fiddling around with my golf clubs while everyone else was playing football - a standard feeling as a medical student.
_________
Back to the Drawing Board
What did I miss? What was going on with Mr. Blue? Who was he, really? These questions kept ping-ponging around inside my brain. I made a mistake with my diagnosis, certainly not uncommon for a student: a great learning experience. However, I was determined to try and understand what was going on; not only for Mr. Blue’s sake but for my own, too.
This meant going back to square one: talking more with Mr. Blue, talking more with the nurses caring for him, diving deeper still into his medical chart…
…but what I found didn’t make things any clearer.
Come back next Wednesday for Part 2
_________
Thank you for reading “Building Docs”! If you enjoyed this article, consider sharing it with friend and family by clicking the button below!
As always, thank you to Dr. Meador who wrote the wonderful book that influences much of my articles and philosophy on “doctoring.” Also, a heartfelt thanks to those members of the medical team I worked with while caring for Mr. Blue. It was some of the greatest training I received during medical school, with the absolute best professionals and teammates.
Sounds like this guy needed a little CME in his life :)